75 year old female patient presented with fever since 2 days and sob since 4 days
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input..
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is
CHEIF COMPLAINTS.
Patient came with cheif complaints of fever since 2 days , shortness of breath since 4 days ,burning micturation since 4 days
HOPI
patient was apparently asymptomatic 4 days back then she developed Shortness of breath since 4 days which was insidious in onset, gradually progressive( from grade 3 to 4) aggrevated on exposure to cold/early morning and relieved on medications
Patient also complains burning micturation not associated with any urgency, frequency/hesitancy
Complaints of fever since 2 days, associated with chills and rigors ,insidious in onset ,high grade no aggrevating factors, and relieved on medications
No c/o chest pain ,orthopnea ,pnd
B/l pitting type of edema. Extending upto knee
PAST HISTORY
patient is k/c/o HTN since 12 years and is on medication TAB.MET XL 50 PO/BD
K/C/O BRONCHIAL ASTHMA since 12 years and is medication
PERSONAL HISTORY
Appetite: normal
Diet:mixed
Sleep: adequate
Bowel and bladder are regular
Patient have past habit of taking tobacco snuff
FAMILY HISTORY:
no history of similar complaints within the family
GENERAL EXAMINATION
Patient is conscious, coherent and cooperative
Well built and we'll nourished
Pallor: absent
Icterus:absent
Clubbing: absent
Cyanosis: absent
Lymphadenopathy: absent
Edema: present ( B/L pedal edema upto knee region)




VITALS:
Temp - 97.5 F
BP 120/80 mmhg
Heart rate 120 bpm
Resp Rate 32/min
Sp02 96%
Grbs 169 mg/ dl
RS
BAE+
NVBS+ ,no crepts
no added sounds
CVS
S1 S2 heard
no murmurs
P/A
soft , tenderness present on suprapubic area,no organomegaly,
CNS
Higher mental functions intact
No focal neurological deficit
PROVISIONAL DIAGNOSIS
?Acute exacerbation of bronchial asthma,
?CAP
?Sepsis secondary to UTI( dengue Igm +)
?Pre renal kidney injury on CKD ( STAGE V)
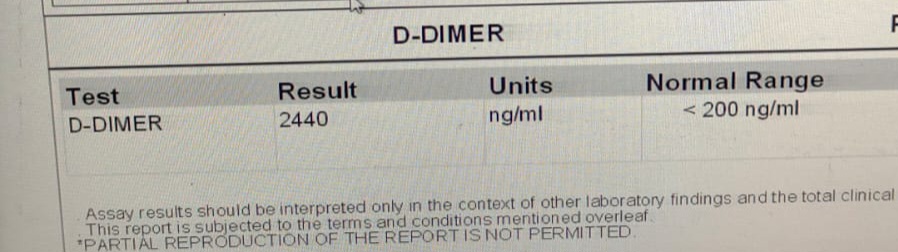
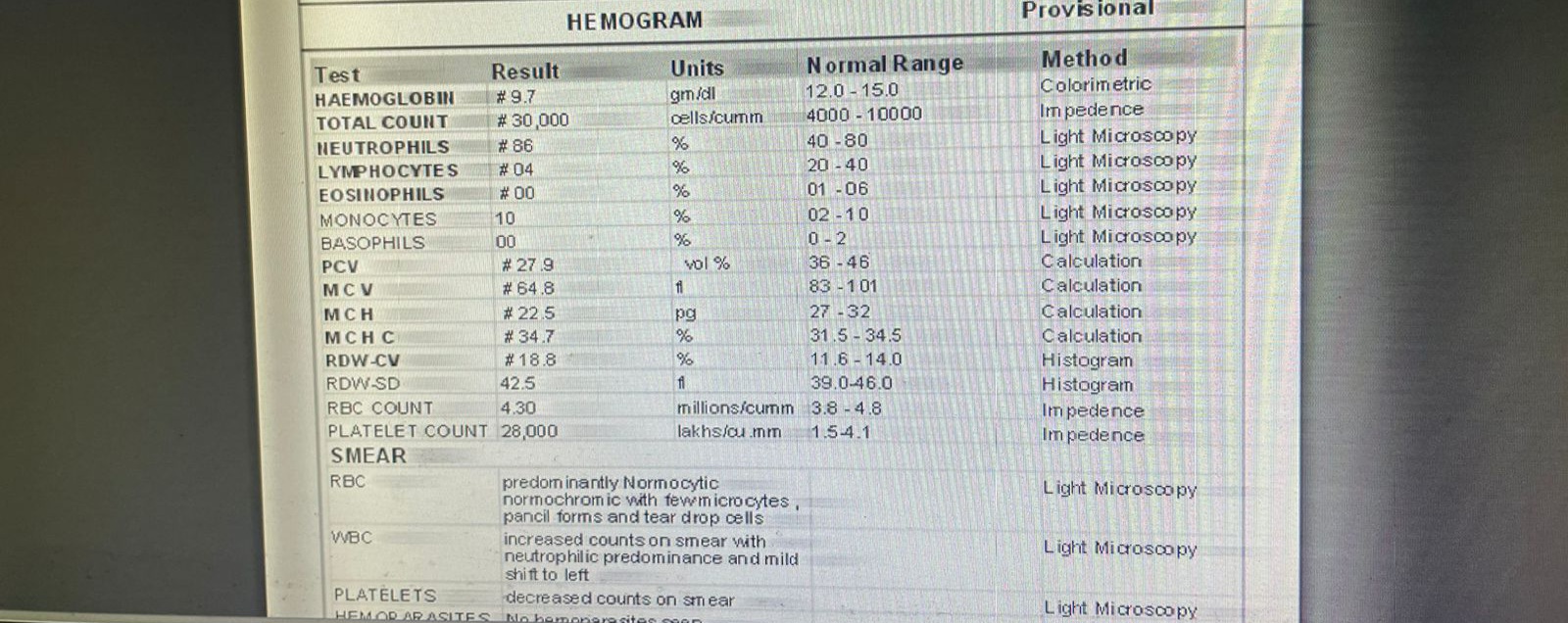
INVESTIGATIONS











Comments
Post a Comment